Melanoma develops from cells in the skin called melanocytes. Melanocytes produce the pigment melanin, which gives skin its color. Melanoma is less common than other skin cancers, such as basal or squamous cell carcinoma, but it is much more deadly.
The incidence of melanoma reported (incidence), in the last 20-30 years has increased significantly. This situation is partially at-risk individuals To UV light strict supervision of exposure of the lesions to be identified and partly due to the increase is due to more early.
Nowadays, as a result of increasing public awareness regarding the early signs of skin melanoma, melanoma is the most captured in the early stages and can be treated surgically.
PATHOGENESIS (GENESIS)
Like other malignant tumors of the skin, melanoma is also mainly UV light-induced DNA damage stems. The gradual acquisition of UV leads to cell mutations.
The incidence of sun-exposed skin, exposure to the sun is high and the majority of the population of light-skinned that are the highest in the geographical regions. Intense intermittent sun exposure at an early age carries the highest risk. Cases of hereditary predisposition also estimated 5% to 10% plays a role in. Individuals with familial melanoma syndrome, a rare US provides valuable information in terms of the study of the development of this tumor.
Family transitive melanomas in 40% of the mitotic division of the cell able to stop CDKN2A Loku germ line mutations in the lobby. This complex locus encodes two tumor suppressor gene. p16, retinoblastoma tumor suppressor protein called the holding cell cycle in the active state G1-S the passage regulating the cyclin-dependent kinase inhibitor. So p16 in the case of normal mitosis G1-S are involved in the control of the phase. p14 with a tumor suppressor p53’s degradation (the breakup) it increases the activity of preventing.
The basic stages of the development of melanoma horizontal and vertical the growth is. The earliest recognizable stage of development of melanoma melanocytes along the dermoepidermal connection has been suggested to occur through the lateral expansion. (lentijinoz hyperplasia and junctional nevus).
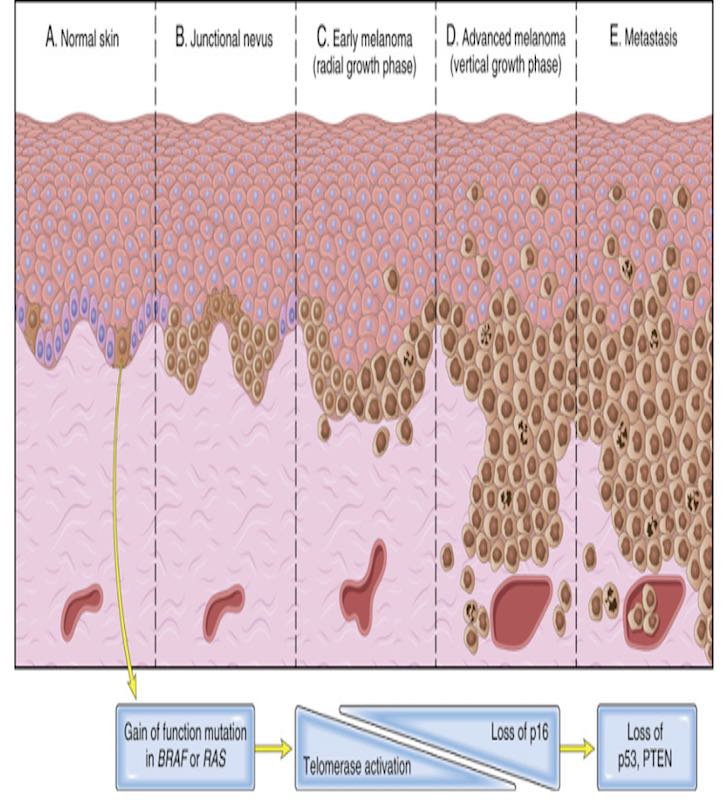
This lesion is then, usually for a long period in the epidermis, with a radial growth phase early melanoma progresses. In this phase melanoma cells invasion and metastasis it is not capable of doing.
Over time, the deeper dermal layers of the tumor mass devoid of cellular maturation as an expanding grew up right down to a vertical growth phase begins. Previously, this event usually flat lesions, is the development of nodules. The emergence of metastatic potential is associated with. Familial and sporadic cases, including cases of benign nevi is seen to result from the DNA sequence, has provided important information on the molecular pathogenesis of melanoma.
Initiator event BRAF or (less commonly) RASin an activating mutation seems to be. In the vast majority of cases, unless it comes to the top of other mutations, this is only produces a benign nevus. Suggestive of melanoma and melanoma, radial growth phase “atypical” morphological characteristics of nevi usually dizilenme with them to activate the expression of telomerase and aging (the usual fate of benign nevi) has shown that mutations that are proposed to stop.
So also with proliferating melanoma cells proliferation, tumor formation in the aging of cells is effective. CDNK2A and p16‘s with additional mutations or epigenetic aberrations, which leads to loss tumors into invasive vertical growth phase shifts. Cutaneous tumor during the phase of evolution, mutation, exposure to UV light increases the burden. Increases the chances of tumor progression.
Finally, REQUIRED and PTEN additional mutations in tumor suppressor genes such as tumor metastasis to the capacity gains. In this phase, aneuploid and genomic copy number changes will occur. This contributes to the genetic heterogeneity of the tumor evolving.
Acral and mucosal melanomas that arise from regions without exposure to the sun is less frequent. This is followed by a different molecular type melanomas. These tumors have a common initiator event KIT receptor tyrosine kinase mutations in the gene function of acquisition. Similarly, in a series of melanomas that arise in the uvea of the eye is the significant driver gene mutations. Most prominent among these is GTP binding with proteins GNAQ or GNA11click is activating mutations.
Sun-exposed melanomas growing in areas with high mutation load. Neoantijen is induced by UV light, forming some of them. From here, suppression of host immune response for the development of melanoma tumor cells (PD-1, PDL-1 and CTLA-4), or should it follows that gain the ability to escape from it.
Many advanced-stage melanomas respond to immune check point inhibitors. These agents silenced melanoma-specific T cells to attack the tumor by releasing they allow. This shows the importance in the development of tumor escape from the immune system.
In summary, the steps to prevent forming a tumor (BRAF, RAS, p16, p14, p53, PTEN) give you the ability to destroy cancer cells and our immune system smart drug treatment treatments for (PD-1, PDL-1 and CTLA-4are known as immune check point inhibitors. Cansi surgery or surgery after non-melanoma in these treatments are widely used. The properties of tumor cells to the use of these treatments should be known. With these features, Pathology Laboratories is unfolded by a series of tests.
MORPHOLOGY (IMAGE)
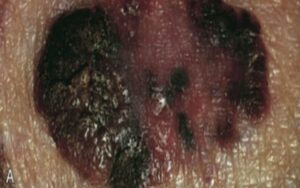
Unlike in benign nevi, melanomas usually black, brown, red, dark blue, and shades of gray, including Exhibit variation in pigmentation. And usually irregular borders “is centikli.”
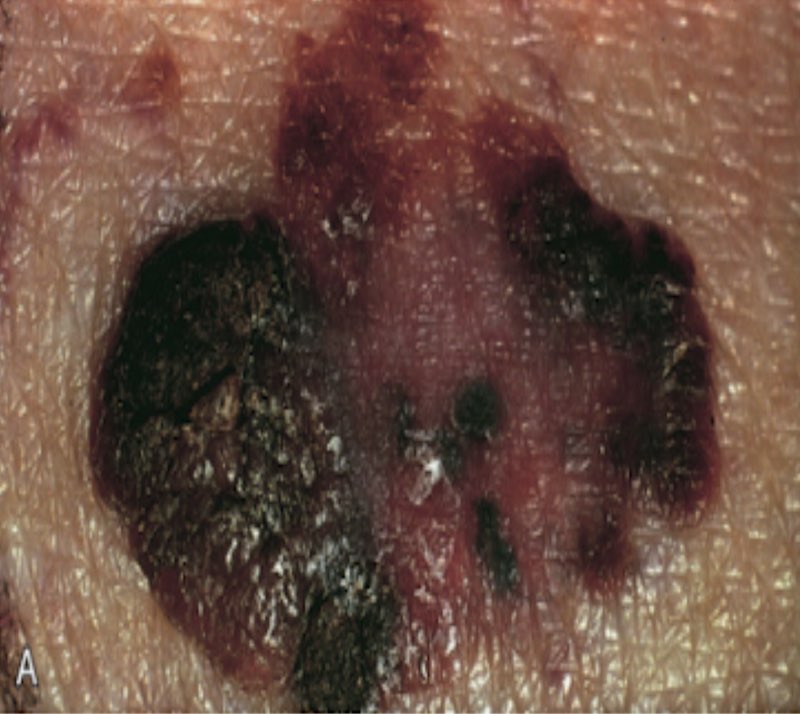
Microscopically, atypical cells at all levels of the epidermis (pagetoid spread) grow as single cells and dermal nodules in expanding slots or badly formed. These are, respectively, the radial (horizontal) and vertical growth phases creates.
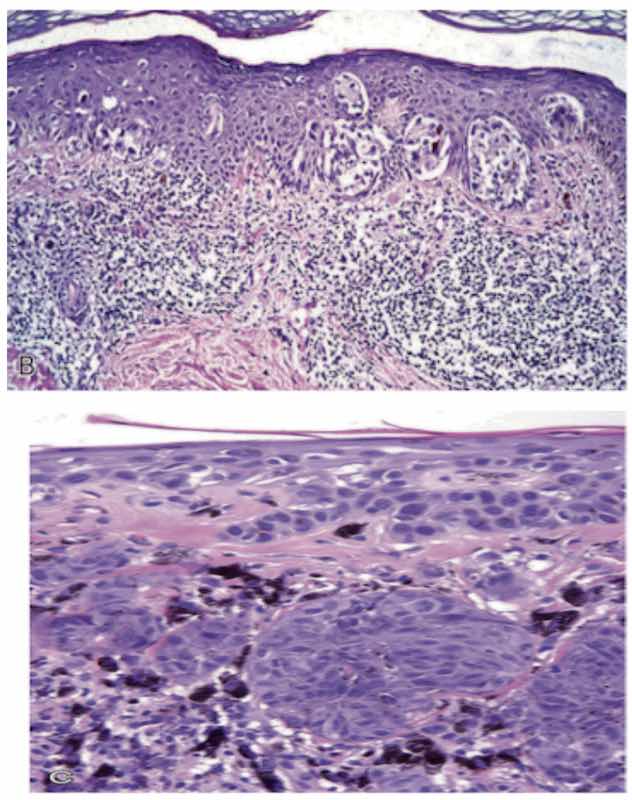
Superficial spreading melanoma is usually in a live lymphoid (immune cells) infiltration facility. This is surrounded by immune cells. This feature is tumor-specific antigens of the host response against suggestive.
At this stage, some proteins in the cells of the tumor and the immune system is activated by the body will be regarded as the damaging agent. The increased thickness of the tumor (vertical growth), biological behavior, is related to a powerful way to worse. Save and get to the bottom of the report a batch of these and other variables (pathology report) gives you the correct information about the behavior of the tumor.
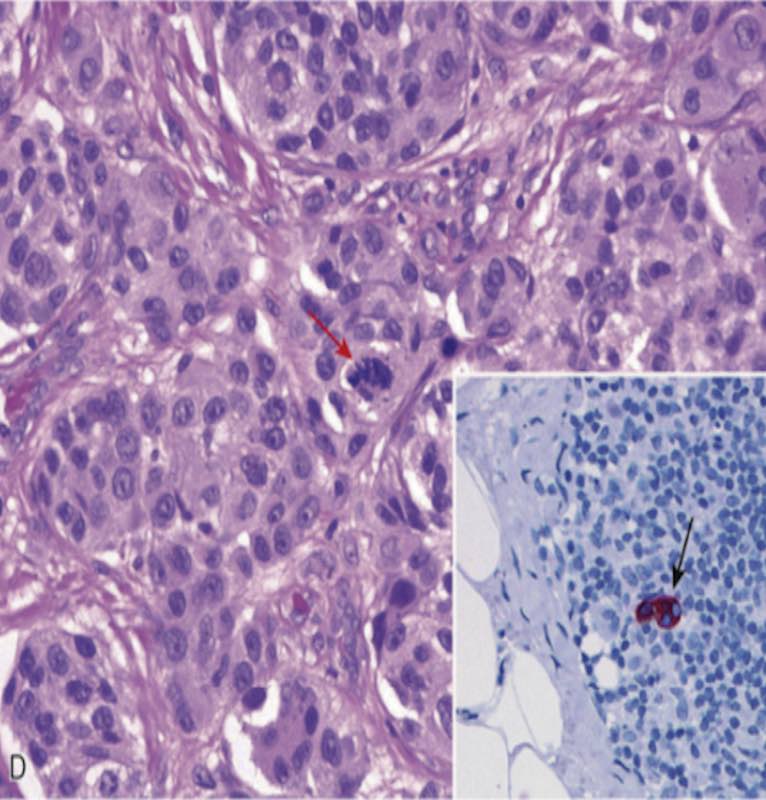
MICROSCOPIC IMAGE
Nevus cells and melanoma cells are usually significantly larger. Irregular typically limited to large kernels, kernel clustered chromatin and prominent characteristic in the vicinity of the membrane as a “cherry-red” superficial eosinophilic most individuals possess. As hmb45 positive immunohistochemical are painted. May help in the identification of metastatic lesions.
CLINICAL FEATURES
Most of these lesions occur in the skin. However, the oral and anogenital mucosal surfaces, ozofagusda the meninges, and in the eye can occur. The incidence of skin melanoma, is inversely proportional to the degree of skin pigmentation. The melanoma is more common in people who have open skin types. Melanoma in people who have darker skin types, the most common soles (called acral melanoma), or in the palm of the nail bed can occur. Important clinical signs, changes in the color or size of a pigmented lesion is.
The main clinical signs include the following:
- A pre-existing mole grow
- Lesions itching or pain,
- New development of a pigmented lesion in adult life
- The irregularity of the boundaries of a pigmented lesion
- A pigmented lesion in a variety of colors
This policy, in the words of melanoma “ABCDE‘s” is expressed:
Asymmetry, border (border) color (color), diameter (diameter) and the change in an existing mole (evolution-evolution)
To know about melanoma and to intervene as quickly as possible is vital. The majority of superficial lesions can be treated surgically, and metastatic melanoma is often fatal.
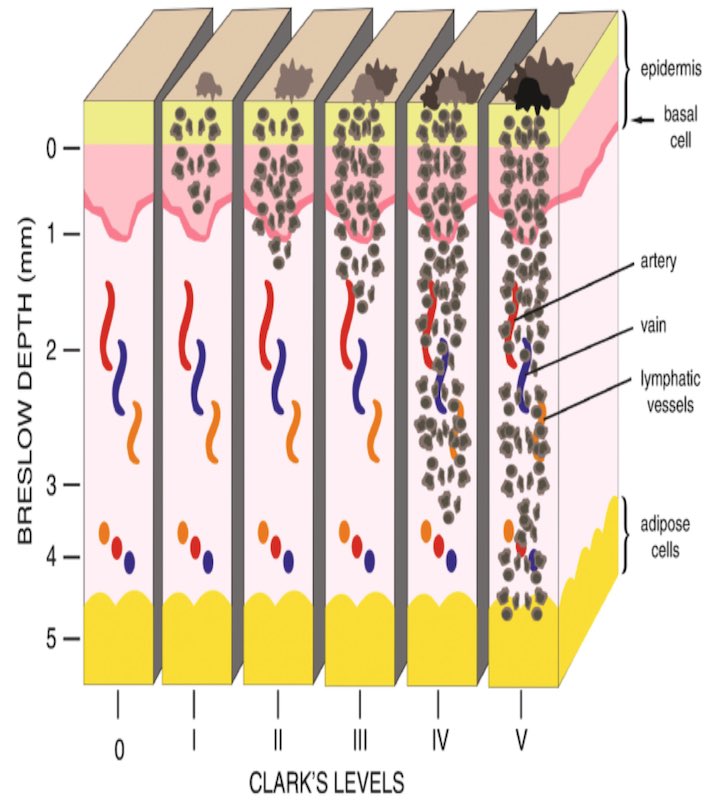
The possibility of metastasis, the upper granular cell layer of the epidermis from the top of the vertical growth phase of nodules is estimated by measuring the depth of invasion in millimeters. Breslow thickness (should be measured as microscopic) is called.
The risk of metastasis, high tumor mitotic rate and local increases in tumors in an immune response without creating. Not only regional metastases to lymph nodes, liver, lungs, and can be seen in every part of the body, including the brain.
Ameliyat sırasında sentinel lenf düğümü biyopsisi (birincil melanomun ilk drene olan düğümünün [düğümlerinin]) biyolojik saldırganlık hakkında ek bilgi sağlar. BRAF and KIT’agents that selectively inhibit i, BRAF and KIT with the dramatic decline in patients with metastatic tumor mutations provides.
However, due to the development of many tumor drug resistance eventually repeats.